


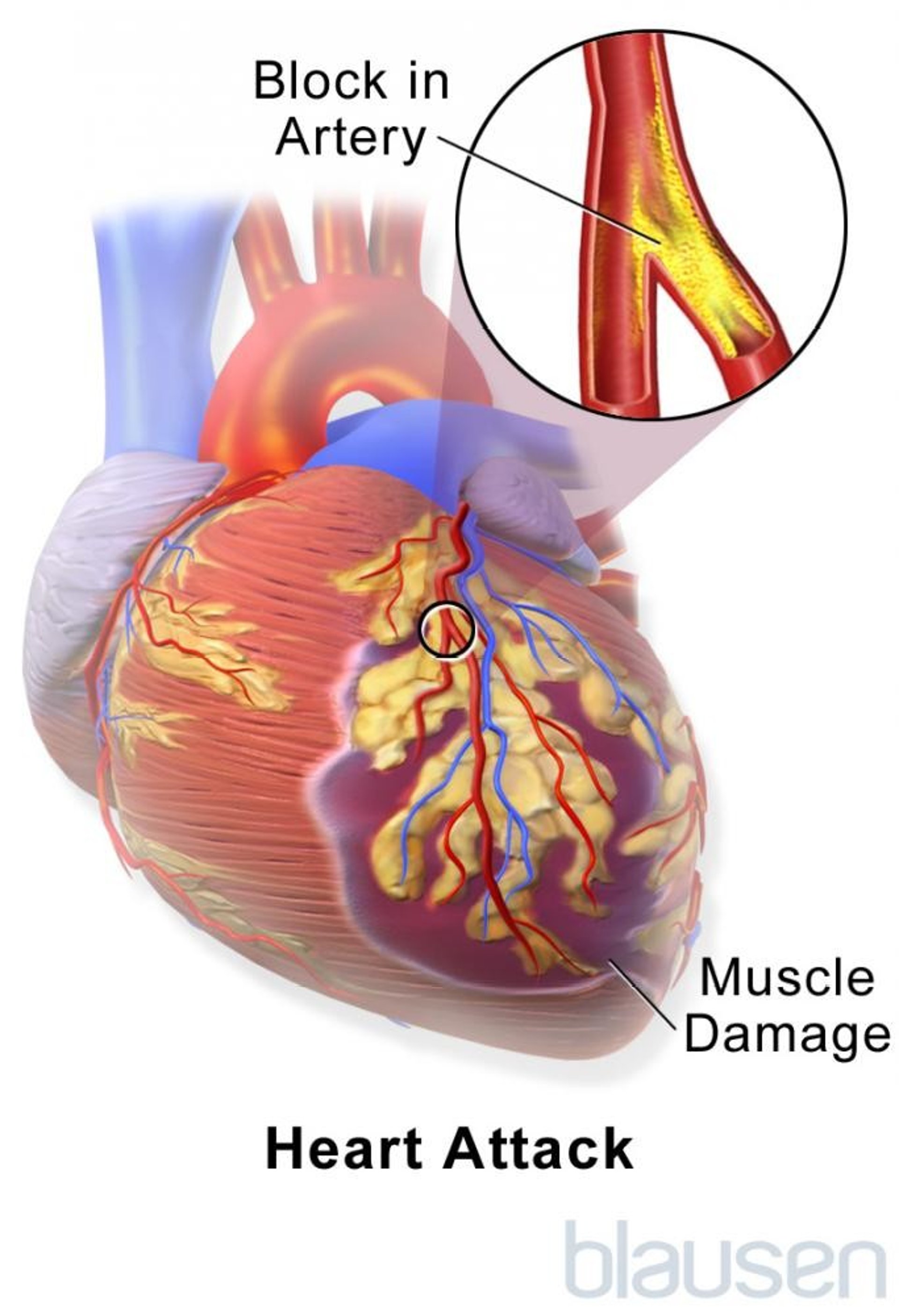
Acute coronary syndromes result from a sudden blockage in a coronary artery. This blockage causes unstable angina or a heart attack (myocardial infarction), depending on the location and amount of blockage. A heart attack is death of heart tissue due to lack of blood supply.
People who experience an acute coronary syndrome usually have chest pressure or ache, shortness of breath, and/or fatigue.
Doctors use electrocardiography and measure substances in the blood to determine whether a person is experiencing an acute coronary syndrome.
Treatment varies depending on the type of syndrome but usually includes attempts to increase blood flow to affected areas of the heart.
(See also Overview of Coronary Artery Disease.)
In the United States, about 1 million heart attacks or sudden cardiac deaths occur each year. And acute coronary syndromes cause almost 400,000 deaths each year.
Causes of Acute Coronary Syndromes
The heart muscle needs a constant supply of oxygen-rich blood. The coronary arteries, which branch off the aorta just after it leaves the heart, deliver this blood. An acute coronary syndrome occurs when a sudden blockage in a coronary artery greatly reduces or cuts off the blood supply to an area of the heart muscle (myocardium). The lack of blood supply to any tissue is termed ischemia. If the blood supply is greatly reduced or cut off for more than a few minutes, heart tissue dies. A heart attack, also termed myocardial infarction (MI), is death of heart tissue due to ischemia.
A blood clot is the most common cause of a blocked coronary artery (see also Overview of Coronary Artery Disease). Usually, the artery is already partially narrowed by a buildup of cholesterol and other fatty materials in the artery wall (atheroma). An atheroma may rupture or tear, which releases substances that make platelets stickier, encouraging clots to form. In about two thirds of people, the blood clot dissolves on its own, typically within a day or so. However, by this time, some heart damage has usually occurred.

Uncommonly, a heart attack results when a clot forms in the heart itself, breaks away, and lodges in a coronary artery. Another uncommon cause is a spasm of a coronary artery that stops blood flow. Spasms may be caused by drugs such as cocaine. Sometimes the cause is unknown.
Classification
Doctors classify acute coronary syndromes based on
The presence of substances in the blood (cardiac biomarkers) released by the damaged heart
Symptoms
Electrocardiography (ECG) results
The classification is important because treatments differ depending on the specific acute coronary syndrome. The classification consists of unstable angina and two types of heart attack.
Unstable angina is a change in the pattern of angina symptoms (chest discomfort), including prolonged or worsening angina and new onset of severe angina symptoms. People who have unstable angina do not have signs of heart attack on their ECG or blood tests.
Non–ST-segment elevation MI is a heart attack that doctors can identify by blood tests but that does not produce typical changes (ST-segment elevation) on an ECG.
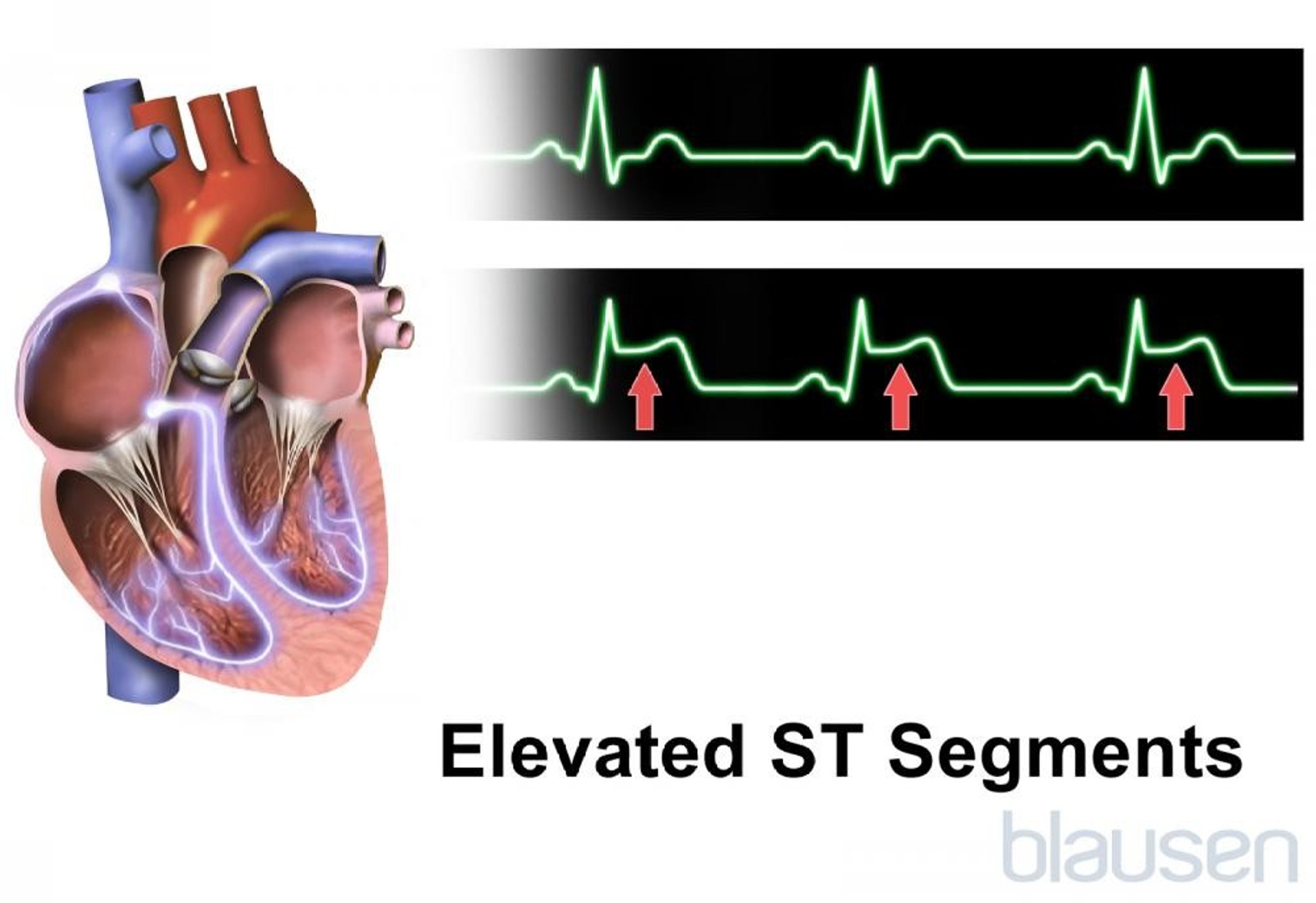
ST-segment elevation MI is a heart attack that doctors can identify by blood tests and also produces typical changes on an ECG (ST-segment elevation) .


Did You Know...
|
Symptoms of Acute Coronary Syndromes
Symptoms of the acute coronary syndromes are similar, and it is usually impossible to distinguish the syndromes based on symptoms alone.
Symptoms of unstable angina are the same as those of angina pectoris—people typically have intermittent pressure, or an ache beneath the breastbone (sternum). People often interpret the sensation as discomfort or heaviness rather than pain. Discomfort also may occur in either shoulder or down the inside of either arm, through the back, and in the throat, jaw, or teeth. However, in people with unstable angina, the pattern changes. People experience more frequent or more severe episodes of angina, or episodes occur at rest or after less physical exertion. About 2 of 3 people who have heart attacks experience unstable angina, shortness of breath, or fatigue a few days or weeks beforehand. Such a change in the pattern of chest pain discomfort may culminate in a heart attack.
With a heart attack,
About one third of people who have a heart attack do not have chest pain. Such people are more likely to be women, people who are not White, those who are older than 75 years, those who have heart failure or diabetes, and those who have had a stroke.
Other symptoms include a feeling of faintness or actually fainting, sudden heavy sweating, nausea, shortness of breath, and a heavy pounding of the heart (palpitations).
During a heart attack, a person may become restless, sweaty, and anxious and may experience a sense of impending doom. The lips, hands, or feet may turn slightly blue or grayish.
Older adults may have unusual symptoms. In many, the most obvious symptom is breathlessness. Symptoms may resemble those of a stomach upset or a stroke. Older adults may become disoriented. Nonetheless, about two thirds of older adults have chest pain, as do younger people. Older adults, especially women, often take longer than younger people to admit they are ill or to seek medical help.
Despite all the possible symptoms, as many as 1 of 5 people who have a heart attack have only mild symptoms or none at all. Such a silent heart attack may be recognized only when ECG is routinely done some time afterward.
During the early hours of a heart attack, heart murmurs and other abnormal heart sounds may be heard through a stethoscope.
Complications
People who have unstable angina or a heart attack may also have complications that can be long-lasting. The complications depend on how much of the heart muscle is damaged, which is a direct result of where a coronary artery was blocked and how long this artery was blocked. If the blockage affects a large amount of heart muscle, the heart will not pump effectively and can become enlarged, possibly leading to heart failure. If the blockage shuts off blood flow to the electrical system of the heart, the heart rhythm may be affected, possibly leading to arrhythmia and sudden death (cardiac arrest).
Diagnosis of Acute Coronary Syndromes
Symptoms
Electrocardiography (ECG)
Blood tests
Whenever a man over age about 30 years or a woman over age about 40 years reports chest pain, doctors usually consider the possibility of an acute coronary syndrome. But several other conditions can cause similar pain, such as pneumonia, a blood clot in the lung (pulmonary embolism), pericarditis, a rib fracture, spasm of the esophagus, indigestion, or chest muscle tenderness after injury or exertion.
ECG and certain blood tests can usually confirm the diagnosis within a few hours.
Electrocardiography
ECG is the most important initial diagnostic test when doctors suspect an acute coronary syndrome. This test provides a graphic representation of the electrical current producing each heartbeat. In many instances, it immediately shows that a person is having a heart attack. Abnormalities detected by ECG help doctors determine the type of treatment needed. The abnormalities on ECG also help show if and where the heart muscle was damaged. If a person has had previous heart problems, which can alter the ECG, the most recent damage may be harder for doctors to detect. Such people should carry a small copy of their ECG, so that if they have symptoms of an acute coronary syndrome, doctors can compare the previous ECG with the current ECG. If a few ECGs recorded over several hours are completely normal, doctors consider a heart attack unlikely.
Cardiac biomarkers
Measuring levels of certain substances (called cardiac biomarkers) in the blood also helps doctors diagnose acute coronary syndromes. These substances are normally found in heart muscle but are released into the blood only when heart muscle is damaged or dead. Most commonly measured are heart muscle proteins called troponin I and troponin T and an enzyme called CK-MB (creatinine kinase, myocardial band subunit). Levels in the blood are elevated within 6 hours of a heart attack and remain elevated for several days. Levels of cardiac markers are usually measured when the person is admitted to the hospital and at 6- to 12-hour intervals for the next 24 hours.
Other testing
When ECG and cardiac marker measurements do not provide enough information, echocardiography or radionuclide imaging may be done. Echocardiography may show reduced motion in part of the wall of the left ventricle (the heart chamber that pumps blood to the body). This finding sometimes suggests damage due to a heart attack.
Other tests may be done during or shortly after hospitalization. These tests are used to determine whether a person needs additional treatment or is likely to have more heart problems. For instance, a person may have to wear a Holter monitor, which records the heart’s electrical activity for 24 hours or more. This test enables doctors to detect whether the person has abnormal heart rhythms (arrhythmias) or episodes of inadequate blood supply without symptoms (silent ischemia). An exercise stress test (electrocardiography done during exercise) before or shortly after discharge can help determine how well the person is doing after the heart attack and whether ischemia is continuing. If these tests detect abnormal heart rhythms or ischemia, medications may be recommended. If ischemia persists, doctors may recommend coronary angiography to evaluate the possibility of doing percutaneous coronary intervention or coronary artery bypass grafting to restore blood flow to the heart.
Treatment of Acute Coronary Syndromes
Medications
Reopening or bypassing blocked arteries
Lifestyle changes
Acute coronary syndromes are medical emergencies. Half of deaths due to a heart attack occur in the first 3 or 4 hours after symptoms begin. The sooner treatment begins, the better the chances of survival. Anyone having symptoms that might indicate an acute coronary syndrome should obtain prompt medical attention. Prompt transportation to a hospital’s emergency department by an ambulance with trained personnel may save the person’s life. Trying to contact the person’s doctor, relatives, friends, or neighbors is a dangerous waste of time.
Did You Know...
|
People who may be having a heart attack are usually admitted to a hospital that has a cardiac care unit. Heart rhythm, blood pressure, and the amount of oxygen in the blood are closely monitored so that heart damage can be assessed. Nurses in these units are specially trained to care for people with heart problems and to handle heart emergencies.
Often, oxygen is given through nasal prongs or a face mask. Providing more oxygen to the heart can help keep heart tissue damage to a minimum.
If no complications occur during the first few days, most people can safely leave the hospital within a few more days. If complications such as abnormal heart rhythms develop or the heart can no longer pump adequately (heart failure), hospitalization can be prolonged.
Medication treatment
aspirin is not taken at home or given by emergency personnel, it is immediately given at the hospital. This therapy improves the chances of survival by reducing the size of the clot (if present) in the coronary artery. People with an allergy to aspirinaspirin and clopidogrel, ticlopidine, or ticagrelor.
People are given medications to prevent the formation of blood clots, to reduce anxiety, and to reduce the size of the heart. People may need to take these medications for some time after they have recovered from a heart attack. Medications are used to reduce the heart's workload during and after a heart attack.
Because decreasing the heart’s workload also helps limit tissue damage, a beta-blocker is usually given to slow the heart rate. Slowing the rate enables the heart to work less hard and reduces the area of damaged tissue.
nitroglycerin
Angiotensin-converting enzyme (ACE) inhibitors can reduce heart enlargement and increase the chance of survival for many people. Therefore, these medications are usually given in the first few days after a heart attack and prescribed indefinitely.
Statins have long been used to help prevent coronary artery disease, but doctors have found that they also have short-term benefit for people with an acute coronary syndrome. Doctors give a statin to people who are not already taking one.
More information on the medications used to treat heart attack can be found in the table Medications Used to Treat Coronary Artery Disease.
Opening the arteries
The decision on the timing and method of opening a blocked coronary artery depends on the type of acute coronary syndrome and on how quickly the person got to the hospital. There are several ways to open blocked coronary arteries:
Clot-dissolving medications
Bypass surgery (coronary artery bypass grafting)
In people who have an ST-segment elevation MI, immediately clearing the coronary artery blockage saves heart tissue and improves survival. Doctors try to clear the blockage within 90 minutes after the person arrives at the hospital. Because the sooner the artery is cleared the better the outcome, the method of clearing is probably not as important as the timing.
Percutaneous coronary interventions (PCI), such as angioplasty and stent placement, appear to be the best way to open blocked arteries during an ST-segment elevation MI if they can be done within 90 minutes of the time the person arrives at the hospital.
Clot-dissolving medications (also called thrombolytic or fibrinolytic medications—see table Medications Used to Treat Coronary Artery Disease
Because thrombolytic medications can cause bleeding, they are not usually given to people who have bleeding in the digestive tract, who have severe high blood pressure, who have recently had a stroke, or who have had surgery during the month before the heart attack.
People who have a non–ST-segment elevation MI or unstable angina do not usually benefit from immediate PCI or thrombolytic medications. However, doctors usually do PCI within the first day or two of hospitalization. If the person’s symptoms worsen or certain complications develop, doctors may do PCI earlier.
In some people, coronary artery bypass grafting (CABG) is done during an acute coronary syndrome instead of using PCI or a thrombolytic medication. For example, CABG may be used for people who cannot be given a thrombolytic medication (for example, because they have a bleeding disorder or have had a recent stroke or recent major surgery). CABG may also be used for people who cannot undergo PCI because of the severity of their arterial disease (for example, because there are many areas of blockage or heart function is poor, especially if the person also has diabetes).
General measures
Smoking is a major risk factor for coronary artery disease, so people who smoke are encouraged to stop smoking.
Stool softeners and gentle laxatives may be used to prevent constipation, so that the person does not have to strain. If the person cannot pass urine or if the doctors and nurses need to keep track of the precise amount of urine produced, a urinary catheter is used.
Discharge
After about 1 to 3 days in the hospital, people who have had an uncomplicated heart attack and successful PCI are usually discharged. Other people may require a longer stay.
lipid-lowering drug (most often, a statin) are usually prescribed.
Rehabilitation
Cardiac rehabilitation, an important part of recovery, begins in the hospital. Remaining in bed for longer than 2 or 3 days leads to physical deconditioning and sometimes to depression and a sense of helplessness. Barring complications, people who have had a heart attack can usually progress to sitting in a chair, passive exercise, use of a commode chair, and reading on the first day. By the second or third day, people are encouraged to walk to the bathroom and engage in nonstressful activities, and they can do more activities each day. If everything goes well, people are usually back to their normal activities within about 6 weeks. Participation in a regular exercise program consistent with the person’s age and heart health is beneficial.
Prognosis for Acute Coronary Syndromes
Many people who have unstable angina go on to have a heart attack within about 3 months.
The most dangerous time for someone who is having a heart attack is during the first few hours, particularly before they arrive at the hospital. Thus, it is critical to seek medical attention immediately when people suspect they are having a heart attack. Most people who survive for a few days after a heart attack can expect a full recovery, but about 10% die within a year. Most deaths occur in the first 3 or 4 months, typically in people who continue to have angina, abnormal heart rhythms originating in the ventricles (ventricular arrhythmias), or heart failure. The prognosis is worse if the heart has enlarged after a heart attack.
Older adults are more likely to die after a heart attack and to have complications, such as heart failure. Women and people with diabetes, hypertension, or overweight are also more likely to have a worse prognosis.
Did You Know...
|
Prevention of Acute Coronary Syndromes
aspirin, or one full adult aspirin daily. Because aspirin prevents platelets from forming clots, it reduces the risk of death and the risk of a second heart attack by 15 to 30%. People with an allergy to aspirinAspirin is not generally recommended for prevention of acute coronary syndrome in people who have not already had a heart attack.
erectile dysfunction, and cold limbs), and not everyone benefits.
Taking lipid-lowering medications will reduce the risk of death after a heart attack.
heart failure, particularly in people who have had a massive heart attack or who develop heart failure.
People should also make changes in their lifestyle. They should eat a low-fat diet and increase the amount of exercise they get. People who have high blood pressure or diabetes should try to keep those disorders under control. People who smoke should quit.






